Erupciones comunes en la infancia
Revisado por pares por Dr Toni Hazell, FRCGPÚltima actualización por Dr Rosalyn Adleman, MRCGPÚltima actualización 7 de mayo de 2025
Cumple con las directrices editoriales
- DescargarDescargar
- Compartir
- Language
- Discusión
- Versión en audio
- Agregar a fuentes preferidas en Google
Profesionales Médicos
Los artículos de Referencia Profesional están diseñados para ser utilizados por profesionales de la salud. Están escritos por médicos del Reino Unido y se basan en evidencia de investigación, así como en guías del Reino Unido y Europa. Puede encontrar el Erupciones cutáneas artículo más útil, o uno de nuestros otros artículos de salud.
Las imágenes de las diversas erupciones pueden estar disponibles haciendo clic en los enlaces. En algunos casos, los enlaces llevan a información factual necesaria para el reconocimiento/gestión de una enfermedad sistémica con manifestaciones dermatológicas. Los recursos en línea en la sección de lecturas adicionales pueden ser útiles para encontrar imágenes adicionales.
Erupciones con lesiones llenas de líquido (vesiculobullosas)
Erupciones con líquido claro
Considere:
Varicela (varicela) - vesicles (initially papules, often not noticed), appearing as 'drops of water'. Superficial, thin-walled with surrounding erythema rapidly changing to pustules and crusts. Appears in crops with all stages represented. Usually begins on the trunk and face before spreading to other parts of the body. Crusts fall off in 1-3 weeks leaving a pink base. Initial fever is classically high before becoming low-grade. Beware of dyspnoea/cough which may indicate varicella-zoster virus (VZV) pneumonitis.
Infección por el virus del herpes simple (VHS) - eczema herpeticum (HSV infection superimposed on pre-existing, often mild, eczema causing an eruption of crusty vesicles and eczematous patches).
Impetigo - this usually takes the form of itchy lesions with macules, vesicles, bullae, pustules and gold-coloured crusts caused by Staphylococcus aureus or group A beta-haemolytic streptococci.
Síndrome de la piel escaldada estafilocócica (SSSS) - appears as blistered scalded skin, due to focal staphylococcal infection releasing an exotoxin.
Necrólisis epidérmica tóxica - an ill-defined red 'burning/painful' macular or papular rash, spreading from the face or the upper trunk. Bullae form and then coalesce. They generally increase in number over 3-4 days (sometimes hours). The epidermis can then slough in sheets. Probably part of a spectrum of disease which includes SSSS and Stevens-Johnson syndrome.
Síndrome de Stevens-Johnson - involves a rash that can begin as macules that develop into papules, vesicles, bullae, urticarial plaques or confluent erythema. The centre of the lesions may be vesicular, purpuric or necrotic. Typically the lesion has the appearance of a target, which is considered pathognomonic. Lesions may become bullous and later rupture.
Eritema multiforme - classically appearing as target lesions (erythematous ring with central vesicle or bulla.)
Pompholyx - an itchy vesicular eruption on the hands and/or feet.
Erupciones pustulosas
Considere:
Acné vulgar - pustules, papules and comedones. Most commonly in teenagers and most commonly on the face but also on the back, shoulders and chest.
Foliculitis - small pustules at the base of hairs.
Erupciones papulares (elevadas)
Considere:
Urticaria - urticaria o sarpullido por ortiga. Un sarpullido rojo elevado, irregular y con picazón. La lesión típica es una pápula o placa blanca central con picazón debido a la hinchazón de la superficie de la piel (roncha). Esto está rodeado por un enrojecimiento eritematoso.
Molusco contagioso - pearly or fleshy, umbilicated (i.e. central depression in papule).
Sarna - itchy, excoriated, S-shaped burrows, which should be visible with a magnifying glass.
Picaduras de insectos - las picaduras suelen resultar en pápulas eritematosas pruriginosas, ya sea individuales o agrupadas. Algunas pueden tener un punto central y otras pueden ser ampollosas. Puede haber una reacción cutánea circundante.
Verrugas virales y verrucae - nódulos o pápulas queratósicas que se encuentran más comúnmente en las manos y los pies.
Queratosis pilaris - keratin accumulation at the base of hair follicles causing a harmless papular skin change.
Milia - common, benign, keratin-filled epidermoid cysts presenting as very small, raised, pearly-white or yellowish bumps on the skin. Common in newborns, but can occur at any age. Usually on the face.
Enfermedad mano-pie-boca - lesions may be papules, vesicles, blisters or ulcers, occurring typically on the oral mucosa and extremities. Most often caused by a member of the Coxsackievirus group.
Erupciones rojas y escamosas
Con ruptura epidérmica (eccematosa)
Eccema atópico typically involves itching erythematous patches, papules and plaques with moist crusted erosions on the face, neck and upper trunk and also the elbows and knees.
Sin ruptura epidérmica
Considere:
Dermatitis seborreica - áreas grasosas inflamadas con descamación fina, más comúnmente en la cara. Se presenta con escamas más gruesas como costra láctea en bebés e infantes.
Psoriasis - psoriasis en placas crónica is typified by itchy, well-demarcated circular-to-oval bright red/pink elevated lesions (plaques) with overlying white or silvery scale, distributed symmetrically over extensor body surfaces and the scalp. (Fissuring within plaques can occur when lesions are present over joint lines or on the palms and soles.)
Tinea corporis - las lesiones cutáneas presentan placas escamosas anulares con bordes elevados. Puede haber vesículas y pústulas.
Tinea capitis - descamación, a menudo con pérdida de cabello, en el cuero cabelludo.
Pitiriasis rosada - generalmente en el tronco. Una placa heráldica de 2-5 cm de diámetro, que es ovalada o redonda con un área central arrugada de color salmón, separada de una zona periférica de color rojo oscuro por escamas finas. Erupción secundaria simétrica con lesiones que son versiones pequeñas de la placa heráldica, con las dos zonas rojas separadas por un anillo escamoso. Por lo general, se distribuyen en un patrón de 'árbol de Navidad'.
Erupciones que son rojas pero no escamosas (y NO púrpuras)
Considere:
Celulitis - infection of the dermis and subcutaneous tissue. There is erythema, pain, swelling and warmth of the affected area.
Enfermedad de Kawasaki - erupción cutánea no vesicular generalizada junto con eritema, hinchazón y descamación que afecta la piel de las extremidades. Asociado con esto hay fiebre que dura ≥5 días, irritabilidad marcada, conjuntivitis bilateral, inflamación de los labios, boca y/o lengua y linfadenopatía cervical.
Fiebre escarlatina y los exantemas virales - por ejemplo:
Sarampión - presents as erythematous macules and papules; initially discrete, may become confluent on the face, neck and shoulders. 2–3 days into the prodromal phase, Koplik spots appear. These are blue-white spots on the inside of the mouth opposite the molars, and occur 24–48 hours before the exantema (rash) stage. The non-itchy rash begins on the face and behind the ears. Within 24–36 hours it spreads over the entire trunk and extremities (palms and soles rarely involved).
Además, infección del tracto respiratorio superior con tos, malestar y fiebre que disminuyen a medida que aumenta la erupción (pródromo del sarampión = las 4 C - tos, coriza, conjuntivitis y muy irritable!).
Fiebre escarlatina (= scarlatina) exotoxin-mediated rash (Group A streptococcus) - sore throat, then general erythema (classically with perioral sparing), followed by confluent petechiae in skin folds (Pastia's sign) due to increased capillary fragility. The skin may have a rough sand-paper feel. Strawberry tongue (initially white, then red). Skin desquamation (peeling) frequently follows the rash.
Rubéola - pink macules and papules starting on the forehead and spreading to the face, trunk and extremities on the first day. Fades from the face on the second day and the rest of the body by the third day. Petechiae on the soft palate before the rash. Low fever.
Erythema infectiosum (slapped cheek syndrome or fifth disease) - caused by parvovirus B19. Hay un eritema dramático en las mejillas, que respeta la nariz, las regiones periorales y periorbitarias. Esto desaparece después de 2-4 días y puede ser seguido por una erupción macular/eritematosa en las extremidades, principalmente en las superficies extensoras. Usualmente no causa picazón en niños pequeños, pero puede causar picazón en niños mayores.
Roseola infantum (sixth disease) - caused by infection with herpesvirus humano 6 (HHV-6) y posiblemente HHV-7. Más común entre los 6 meses y 1 año de edad.
Erupciones que son rojas y purpúricas
Considere:
Meningitis meningocócica (not the most common but it must be excluded). Early on there may be a 2-10 mm macular or maculopapular rash (becoming apparent within the first 24 hours of disease) which is sparsely distributed on the face, trunk and lower extremities and blanches on pressure. Later as the disease develops, petechiae in the centre of macules become haemorrhagic (and do not blanche). Use the 'glass test' to assess 'blanchability' of the rash by placing a glass tumbler against lesions and applying pressure.
Púrpura de Henoch-Schönlein - vasculitis por hipersensibilidad autoinmune en la infancia. Las principales características clínicas son púrpura cutánea, artritis, dolor abdominal, sangrado gastrointestinal, orquitis y nefritis.
Immune thrombocytopenia (ITP) - condición autoinmune que resulta en un bajo número de plaquetas circulantes, causando petequias y hematomas y, menos comúnmente, sangrado interno más grave.
Leucemia and other haematological disorders.
Trauma and non-accidental injury (NAI).
Algoritmo
Resumen de Erupciones Cutáneas Pediátricas
Algoritmo de Erupciones
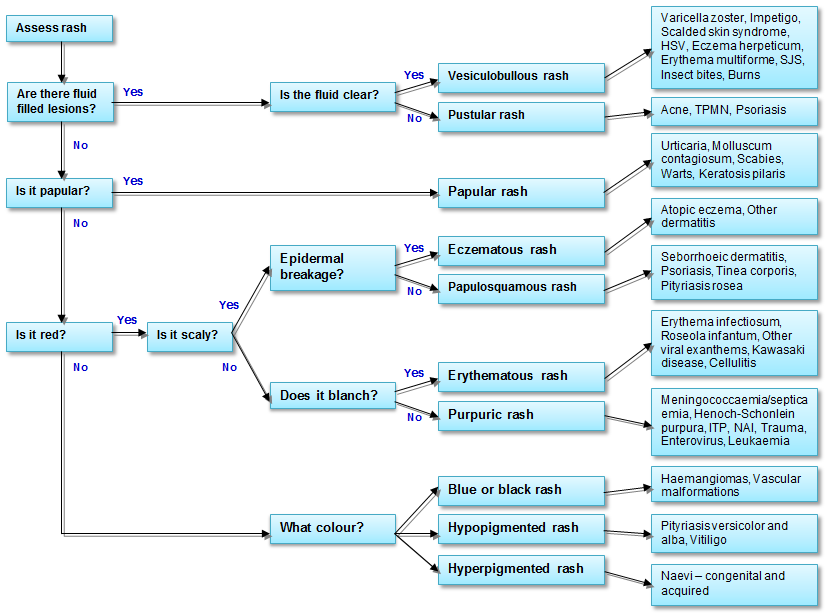
© Adaptado por el Dr. Adrian M Bonsall, del Manual de Pediatría 6ª Ed. Hospital de Niños Royal, Melbourne
Notas al pie1 2
La lista completa de los exantemas originales es:
Primera enfermedad = sarampión, o rubeola.
Segunda enfermedad = fiebre escarlatina, o escarlatina.
Tercera enfermedad = sarampión alemán, o rubéola.
Cuarta enfermedad = enfermedad de Dukes, o enfermedad de Filatov.
Quinta enfermedad = síndrome de mejilla abofeteada, o eritema infeccioso.
Sexta enfermedad = exantema súbito, o roséola infantil.
This ordinal nomenclature came about because, at the turn of the century, there were classically three exanthematous diseases recognised: measles, rubella and scarlet fever. Then, in 1900, Dr. Clement Dukes, medical officer at Rugby School, described another exanthem which he called 'fourth disease'.
In 1905 erythema infectiosum (a term already in use for six years applying to the disease described previously by Tshamer and later by Escherich) was the fifth disease added to the list. Later, sixth disease (roseola infantum) was recognised and fourth disease was rejected by most observers because of insufficient evidence to support its existence as an independent entity.
Así que las enfermedades primera, segunda, tercera y sexta ahora se conocen por sus nombres más comunes, dejando la quinta enfermedad como un recordatorio solitario de los días en que, sin la ayuda de la microbiología sofisticada, los clínicos-epidemiólogos observadores eran capaces de categorizar un grupo de exantemas confusos.
Actualizaciones exclusivas para profesionales de la salud
Mantente informado con las últimas actualizaciones clínicas, perspectivas profesionales y orientación basada en evidencia. El boletín de Patient Pro selecciona contenido esencial para profesionales de la salud, entregado directamente en tu bandeja de entrada.
Al suscribirte aceptas nuestros Política de Privacidad. Puedes darte de baja en cualquier momento. Nunca vendemos tus datos.
Lecturas adicionales y referencias
- Sladden MJ, Johnston GA; Infecciones cutáneas comunes en niños. BMJ. 2004 Jul 10;329(7457):95-9.
- Sladden MJ, Johnston GA; Infecciones cutáneas más comunes en niños. BMJ. 21 de mayo de 2005;330(7501):1194-8.
- DermNet NZ
- DermIS - Sistema de Información de Dermatología
- Drago F, Ciccarese G, Gasparini G, et al; Exantemas infecciosos contemporáneos: una actualización. Future Microbiol. 2017 Feb;12:171-193. doi: 10.2217/fmb-2016-0147. Epub 2016 Nov 14.
- Weisse M; La cuarta enfermedad, 1900-2000 The Lancet 2001; 357:299-301.
Sobre el autorVer biografía completa

Dr Rosalyn Adleman, MRCGP
MRCGP
La Dra. Rosalyn Adleman es una médica de cabecera del NHS que trabaja en el norte de Londres.
Acerca del revisorVer biografía completa

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
La Dra. Toni Hazell se graduó de la Escuela de Medicina del Hospital St. Mary y realizó su VTS en el Hospital Northwick Park.
Historial del artículo
La información en esta página está escrita y revisada por pares por clínicos calificados.
Artículo también disponible en Inglés, Alemán, Español, Francés, Italiano, Portugués, Hindi, Hebreo, Árabe, y Sueco.
Próxima revisión: 6 de mayo de 2028
7 de mayo de 2025 | Última versión

Pregunta, comparte, conecta.
Navega por discusiones, haz preguntas y comparte experiencias en cientos de temas de salud.

¿Te sientes mal?
Evalúa tus síntomas en línea de forma gratuita
Más en pediatría
- Asma
- Trastornos del espectro autista
- Lesiones de nacimiento en el bebé
- Bronquiolitis
- Cetoacidosis infantil
- Malformaciones urogenitales congénitas
- Fibrosis quística
- Diagnóstico del asma infantil en atención primaria
- Problemas oculares en bebés
- Enfermedad fabricada o inducida por cuidadores
- Alergia alimentaria e intolerancia alimentaria
- Galactosemia
- Alimentación infantil
- Neuroblastomas
- Oftalmia neonatal
- Enfermedad de Osgood-Schlatter
- Alivio del dolor en niños
- Deficiencia primaria de anticuerpos
- Pequeño para la edad gestacional