Úlceras venosas en las piernas
Revisado por pares por Dr Colin Tidy, MRCGPÚltima actualización por Dr Hayley Willacy, FRCGP Última actualización 26 Sept 2023
Cumple con las directrices editoriales
- DescargarDescargar
- Compartir
- Language
- Discusión
- Versión en audio
- Agregar a fuentes preferidas en Google
En esta serie:Venas varicosasEczema varicosoTromboflebitis superficial
Las úlceras venosas en las piernas son comunes en personas mayores. La parte más importante del tratamiento es que un enfermero aplique correctamente las vendas de compresión. Mantente lo más activo posible, pero eleva la pierna cuando estés descansando. En algunos casos, se pueden recomendar otros tratamientos, como un injerto de piel o cirugía de venas. Después de que una úlcera haya sanado, debes usar una media de soporte cada día, lo que ayuda a prevenir que vuelva a aparecer.
De un vistazo
A venous leg ulcer is a skin break that mainly occurs just above the ankle.
It happens when increased blood pressure in leg veins damages the skin, causing an ulcer.
The diagnosis involves checking blood pressure in your ankle and arm to rule out other causes.
Compression bandaging and keeping your leg raised are key treatments for healing.
Most ulcers heal within 12 weeks with weekly compression bandaging.
To prevent recurrence, wear a compression stocking daily for at least five years after healing.
See your doctor or nurse if you have increasing pain or changes in your foot colour or temperature while wearing bandages.
What is a venous leg ulcer?
A skin ulcer develops when an area of skin breaks down to reveal the underlying flesh. Venous leg ulcers are the most common type of skin ulcer. They mainly occur just above the ankle. They usually affect older people and are more common in women.
Varicose ulcer
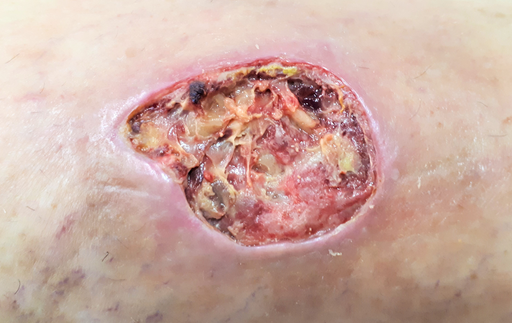
© Raimundo Pastor, CC BY-SA 4.0, via Wikimedia Commons
Chronic venous insufficiency & Venous ulcer

© Ashashyou, CC BY-SA 4.0, via Wikimedia Commons
How common are leg ulcers?
Venous leg ulcers are the most common type of leg ulcer, causing about 3 in 4 of all leg ulcers. They affect about 1 in 100 people in the UK at some stage in their lives. Venous leg ulcers become more common as you get older. Most are painless but some are painful. Without treatment, an ulcer may become larger and cause problems in the leg. Skin inflammation (dermatitis) sometimes develops around a venous ulcer.
Non-venous skin ulcers are less common. For example, a skin ulcer may be caused by poor circulation due to artery disease in the leg, problems with nerves that supply the skin, or other problems. The treatment for non-venous ulcers is different to that of venous ulcers.
The rest of this leaflet deals only with venous leg ulcers.
What causes venous leg ulcers?
The root of the problem is increased pressure of blood in the veins of the lower leg. This causes fluid to ooze out of the veins beneath the skin. This causes swelling, thickening and damage to the skin. The damaged skin may eventually break down to form an ulcer.
The increased pressure of blood in the leg veins is due to blood collecting in the smaller veins next to the skin. The blood tends to collect and pool because the valves in the larger veins become damaged by a previous blood clot (trombosis) in the vein, or las venas varicosas. Gravity causes blood to flow back through the damaged valves and pool in the lower veins.
How is a venous leg ulcer diagnosed?
The appearance of a venous leg ulcer is usually fairly typical. It often looks different to ulcers caused by other problems such as poor circulation or nerve problems.
To rule out poor circulation as a cause, it is usual for a doctor or nurse to check the blood pressure in the ankle y in the arm. The ankle blood pressure reading is divided by the arm blood pressure reading to give a blood pressure ratio called the Ankle Brachial Pressure Index (ABPI).
If the ratio is low (less than 0.8) it indicates that the cause of the ulcer is likely to be poor circulation (peripheral arterial disease) rather than venous problems. This is very important to know as the treatments are very different. An ABPI may be checked every six months or so to make sure the circulation to the legs remains good.
Certain blood and urine tests may also be done to rule out conditions such as anemia, diabetes, problemas renales y artritis reumatoide, which may cause or aggravate certain types of skin ulcer.
In complicated cases you may need to have an ultrasonido, tomografía computarizada o resonancia magnética to produce a detailed map of the blood circulation in your leg.
Venous leg ulcer treatment
The ulcer is dressed in a similar way to any other wound. Typically, a nurse will do this every week or so. The wound is cleaned when the dressing is changed - normally with ordinary tap water. However, an ulcer is unlikely to heal with just dressings. In addition to a dressing, the following treatments help the ulcer to heal.
Compression bandaging
Wearing a compression bandage is the most important part of treatment. The aim is to counteract the raised pressure in the leg veins. This gives the best chance for the ulcer to heal. The common method is for a nurse to put on 2-4 layers of bandages over the dressing. When the bandages are put on, the pressure is put highest at the ankle and gradually less towards the knee and thigh. A support (compression) stocking over the dressing is sometimes used as an alternative but not thought to be as good as bandaging.
The bandages are reapplied every week or so. It is best to put the bandages on after you have raised (elevated) the leg for several hours or overnight (see below). So, make extra effort to keep your leg elevated just before the nurse is due to see you.
A note of caution: when you have a compression bandage on you should still be able to move your ankle around. Occasionally, the compression is too tight, or it may affect the circulation in the legs. Therefore, take off the bandages if your foot changes colour or temperature, or if you have increasing pain. Then see your doctor or nurse for advice.
Elevation and activity
When you are resting, if possible, try to keep your leg raised higher than your hip. This is particularly important if your leg is swollen. The aim is to let gravity help to pull fluid and blood in the right direction - towards the heart. This reduces swelling in the leg and reduces the pressure of blood in the leg veins.
Try to set 3 or 4 periods per day of about 30 minutes to lie down with your leg raised. For example, lie on a bed or sofa with your foot on a couple of pillows. However, do not spend all your time in bed or resting. For the rest of the time, keep as active as you can and do normal activities. If possible, regular walks are good but do not stand still for long periods.
When you sleep overnight, if possible, try to keep your leg raised. You can do this by putting some pillows under the bottom of the mattress. (It may not be possible to sleep like this if you have certain other medical problems or disabilities.)
Otros tratamientos
In some people, other conditions such as anemia, poor nutrition, swelling of the legs and other medical problems may mean that the skin has less chance of healing well. Other treatments may be needed to help heal a venous leg ulcer - for example:
Try to stop smoking if you are a smoker. The chemicals in cigarettes may interfere with the skin healing.
Medicamentos antibióticos are sometimes advised for short periods if the skin and tissues around the ulcer become infected.
Analgésicos can be taken if the ulcer is painful.
Skin care. The skin around an ulcer is often inflamed or scaly. Your doctor or nurse may advise on a cream to reduce inflammation if necessary.
Consejos dietéticos if your diet is not very good. Also, if you are overweight then perder peso may help. Obesity is a risk factor for developing venous leg ulcers.
Iron tablets or other treatments if you are anaemic.
Pentoxifylline improves blood circulation and you may be offered this medicine to promote healing of the ulcer.
Hyperbaric oxygen (oxygen delivered at high pressure) is sometimes used when facilities are available.
A skin graft may be advised for a large ulcer, or for one that does not heal well.
Cirugía for las venas varicosas or other vein problems is advised in some cases. This may correct back pressure of blood pooling in the veins and allow an ulcer to heal.
The topical haemoglobin spray (Granulox®) is a medical device to be used in the treatment of chronic wounds, such as venous leg ulcers. It works by increasing the oxygen supply to the wound, to speed up the healing process. Granulox® is now available to specialist wound care teams in hospitals and in the community.
¿Cuál es el pronóstico?
Up to 7 in 10 venous ulcers heal within 12 weeks if treated with compression bandaging which is reapplied every week or so. If compression is not used and an ordinary dressing or support (compression) stockings alone are used, the chance of healing is less.
Preventing a recurrence of venous skin ulcers
Venous leg ulcers commonly come back (recur) after they have healed. To prevent this, you should wear a support (compression) stocking during the daytime for at least five years after the ulcer has healed. This counteracts the raised pressure in the veins that causes venous leg ulcers.
You should get a new stocking about every six months as the elastic tends to go after a while. Special stockings (compression stockings) can be prescribed or bought at pharmacies. They come in different sizes - your pharmacist will advise. Compression stockings for the prevention of venous leg ulcers are usually below knee in length rather than thigh length.
There are different strengths (classes) of compression stockings - class 1, 2 and 3. The higher the class (class 3) the greater the compression. Ideally, wear class 3 stockings. However, some people find class 3 stockings too tight and uncomfortable but class 2 may be fine. It is still better to wear some sort of compression stocking than none at all.
Nota: proper compression stockings used for medical purposes are different to the support stockings or tights sold in ordinary clothing shops.
A leg ulcer is much less likely to recur if you wear compression stockings regularly.
Sometimes surgery for varicose veins or other vein problems is advised after an ulcer has healed, in order to help prevent a recurrence.
Selecciones del paciente para Venas

Salud del corazón y vasos sanguíneos
Venas varicosas
Los estudios sugieren que las venas varicosas ocurren en 10-20 de cada 100 hombres y 25-33 de cada 100 mujeres. La mayoría de las personas con venas varicosas no tienen una enfermedad subyacente. A menudo ocurren sin una razón aparente, aunque en algunos casos están asociadas con factores de estilo de vida. Las venas varicosas no causan síntomas ni complicaciones en la mayoría de los casos, aunque algunas personas las encuentran poco estéticas. Si se aconseja el tratamiento, o se desea por razones estéticas, se utiliza un procedimiento para sellarlas. Hay varios procedimientos disponibles: calor, láseres o productos químicos inyectados en las venas. Estos métodos han reemplazado en gran medida los métodos quirúrgicos anticuados como la extracción de las venas.
por el Dr. Colin Tidy, MRCGP

Salud del corazón y vasos sanguíneos
Trombosis venosa profunda
Una trombosis venosa profunda (TVP) es un coágulo de sangre en una vena. Los coágulos de sangre en las venas ocurren con mayor frecuencia en las piernas, pero pueden ocurrir en otras partes del cuerpo, incluidos los brazos. Este folleto trata sobre los coágulos de sangre en las venas de las piernas. La causa más común de que se desarrolle un coágulo de sangre en una vena es la inmovilidad. En algunos casos, puede ocurrir una complicación donde parte del coágulo de sangre se desprende y viaja al pulmón (embolia pulmonar). Esto generalmente se previene si se le administra tratamiento anticoagulante.
por la Dra. Toni Hazell, MRCGP
Preguntas frecuentes
What is the difference between an ordinary dressing and compression bandaging for a leg ulcer?
An ordinary dressing is used to cover and clean the wound, similar to any other wound. However, for a venous leg ulcer, compression bandaging is specifically applied in addition to the dressing. Compression bandaging is the most crucial part of treatment as it counteracts the increased pressure in the leg veins, which is the underlying cause of these ulcers, giving them the best chance to heal. Without compression, the ulcer is less likely to heal.
My job requires me to stand for long periods. How can I manage my leg ulcer?
While it's important to keep active and continue with normal activities, standing still for long periods should be avoided if you have a venous leg ulcer. When you are resting, you should try to elevate your leg higher than your hip for about 30 minutes, three or four times a day. This helps reduce swelling and pressure in the leg veins. You should also consider wearing compression bandages as prescribed, which counteract the high pressure in the veins.
What is the role of diet and weight in managing venous leg ulcers?
If your diet is not good, dietary advice may be needed as poor nutrition can hinder the skin's ability to heal. Additionally, if you are overweight, losing weight may help. Obesity is recognised as a risk factor for developing venous leg ulcers.
How do compression stockings used for preventing recurrence differ from regular support stockings?
Proper compression stockings, used for medical purposes to prevent venous leg ulcer recurrence, are specifically designed with different strengths and provide consistent graduated compression highest at the ankle. These are different from the general support stockings or tights sold in ordinary clothing shops, which do not offer the same level of therapeutic compression.
How can I tell if my compression bandage is too tight?
You should still be able to move your ankle around when wearing a compression bandage. If the compression is too tight, or if it starts to affect the circulation in your legs, you might notice your foot changing colour or temperature, or experience increasing pain. In such cases, you should remove the bandages and seek advice from your doctor or nurse.
Lecturas adicionales y referencias
- Bonkemeyer Millan S, Gan R, Townsend PE; Venous Ulcers: Diagnosis and Treatment. Am Fam Physician. 2019 Sep 1;100(5):298-305.
- Medias de compresión; NICE CKS, mayo 2022 (acceso solo en el Reino Unido)
- Norman G, Westby MJ, Rithalia AD, et al; Dressings and topical agents for treating venous leg ulcers. Cochrane Database Syst Rev. 2018 Jun 15;6(6):CD012583. doi: 10.1002/14651858.CD012583.pub2.
- Cullum N, Liu Z; Therapeutic ultrasound for venous leg ulcers. Cochrane Database Syst Rev. 2017 May 15;5(5):CD001180. doi: 10.1002/14651858.CD001180.pub4.
- Keohane C, Westby D, Nolan FC, et al; Hyperbaric Oxygen as an Adjunct in the Treatment of Venous Ulcers: A Systematic Review. Vasc Endovascular Surg. 2023 Mar 8:15385744231162924. doi: 10.1177/15385744231162924.
- Úlcera de pierna - venosa; NICE CKS, julio 2023 (acceso solo en el Reino Unido)
Sobre el autorVer biografía completa

Dr Hayley Willacy, FRCGP
Médico General, Autor Médico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dra. Hayley Willacy fue una médica general del NHS que trabajaba en el noroeste de Inglaterra, quien se retiró de la práctica clínica en 2022 después de 30 años.
Acerca del revisorVer biografía completa

Dr Colin Tidy, MRCGP
Médico General, Autor Médico
MBBS, MRCGP, MRCP (Paediatrics), DCH
El Dr. Colin Tidy es un médico del NHS, con sede en Oxfordshire.
Historial del artículo
La información en esta página está escrita y revisada por pares por clínicos calificados.
Artículo también disponible en Inglés, Alemán, Español, Francés, Italiano, Portugués, Hindi, Hebreo, Árabe, y Sueco.
Próxima revisión: 24 de septiembre de 2028
26 Sept 2023 | Última versión

Pregunta, comparte, conecta.
Navega por discusiones, haz preguntas y comparte experiencias en cientos de temas de salud.

¿Te sientes mal?
Evalúa tus síntomas en línea de forma gratuita
Suscríbete al boletín de Patient
Tu dosis semanal de consejos de salud claros y confiables, escritos para ayudarte a sentirte informado, seguro y en control.
Al suscribirte aceptas nuestros Política de Privacidad. Puedes darte de baja en cualquier momento. Nunca vendemos tus datos.
Más sobre la salud del corazón y los vasos sanguíneos
- Aneurisma aórtico abdominal
- Electrocardiograma ambulatorio
- Angina
- Disección aórtica
- Fibrilación auricular
- Betabloqueantes
- Cateterismo cardíaco
- Enfermedad cardíaca congénita
- Insuficiencia cardíaca congestiva
- Espasmo de la arteria coronaria
- Ecocardiograma
- Electrocardiograma
- ataque al corazón
- Palpitaciones del corazón
- Presión arterial alta
- Registro de presión arterial en casa y ambulatoria
- Endocarditis infecciosa
- Vivir con presión arterial alta
- Escaneo de perfusión miocárdica
- Tromboflebitis superficial