Tummy tuck
Abdominoplasty
Peer reviewed by Dr Helen Huins, MRCGPLast updated by Dr Jacqueline Payne, FRCGPLast updated 24 Mar 2016
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
This page has been archived.
It has not been reviewed recently and is not up to date. External links and references may no longer work.
In this procedure excess skin and fat can be removed, abdominal contours and scars improved, and the muscles tightened.
At a glance
Abdominoplasty is a surgical procedure to remove excess skin and fat from the abdomen.
There are different types of abdominoplasty, including standard, mini, extended, and endoscopic.
The procedure typically leaves a long scar across the lower abdomen, sometimes with a scar around the navel.
Numbness and swelling in the lower abdomen are common after surgery.
Best results are seen in people who are a healthy weight.
You will need to stop taking the contraceptive pill and stop smoking before surgery to reduce risks.

This leaflet is provided by the British Association of Aesthetic Plastic Surgeons, the professional body responsible for the advancement of education and safety in aesthetic plastic surgery.
This is also called an abdominoplasty or tummy tuck. Different combinations are combined in the various procedures.
The standard abdominoplasty
Standard abdominoplasty
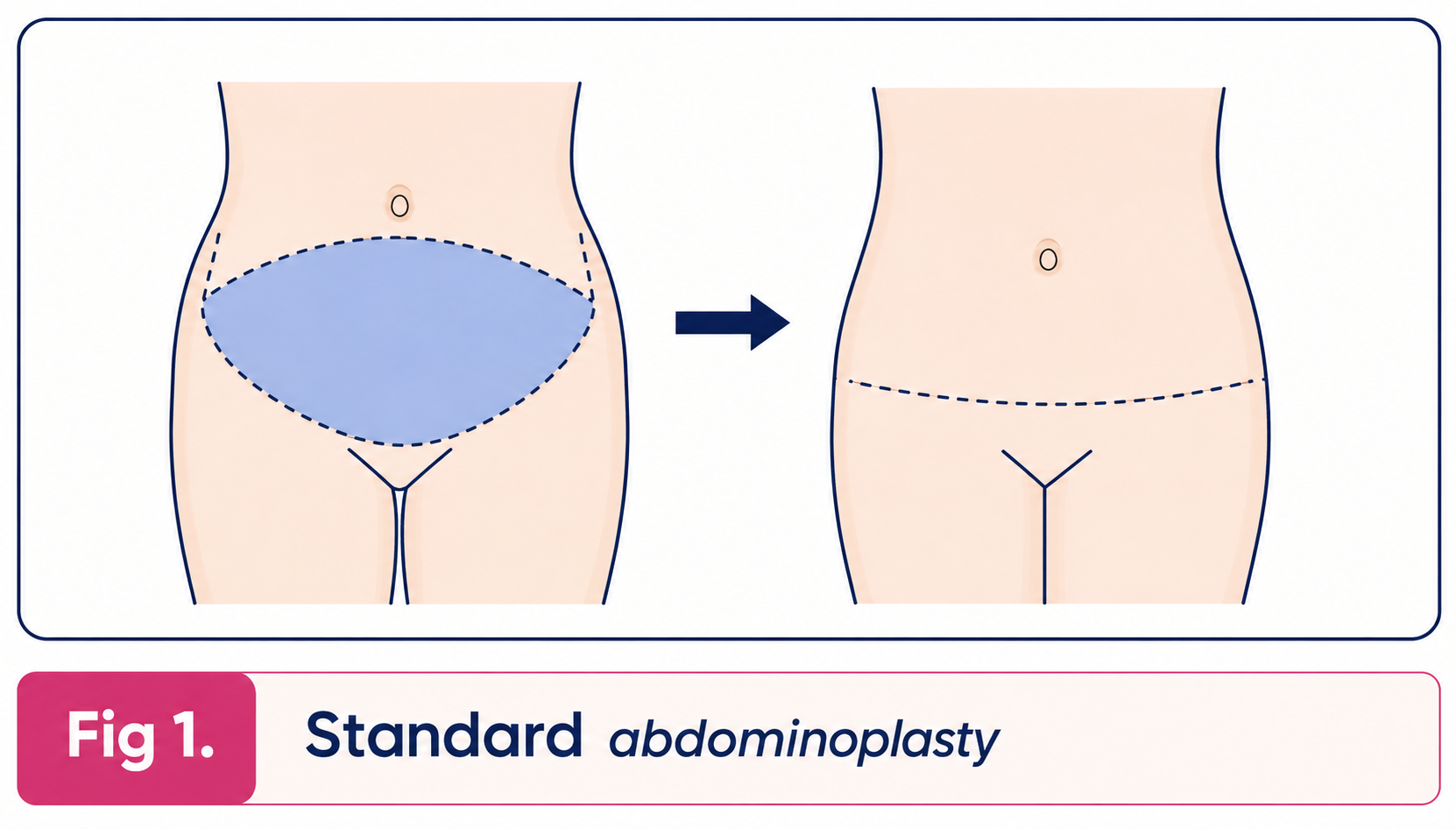
The excess skin and fat of the abdominal wall between the pubic area and the umbilicus (navel) is removed leaving the umbilicus in place. The skin of the abdominal wall at the level of the umbilicus is then drawn down to suture it at the pubic level. The patient is left with a long, usually curved scar across the lower part of the abdominal wall at the level of the pubic hair. There is also a scar around the umbilicus. Any looseness of the muscles of the abdominal wall or hernia is repaired at the same time.
Liposuction may be carried out during this procedure to thin the abdominal wall, or as a separate procedure either before or after the abdominoplasty.
Mini abdominoplasty
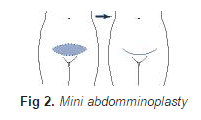
In the mini-abdominoplasty surplus skin below the umbilicus is removed leaving a low abdominal scar at the level of the pubic hair. The umbilicus is not disturbed but liposuction is usually carried out at the same time as the procedure to reduce the thickness of fat in the abdominal wall and any laxity or hernia of the abdominal wall is repaired at the same time.
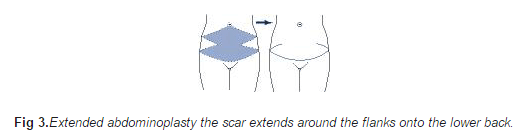
In the extended abdominoplasty surplus skin and fat of the loins and back are also removed so that the scar extends around the flanks on to the lower back.
Extended abdominoplasty
The endoscopic abdominoplasty is used to tighten the muscles of the abdominal wall to give a better contour and is carried out through a short transverse incision above the pubic hair. Skin is not removed but liposuction can be carried out at the same time.
The apronectomy is a modification of the mini-abdominoplasty for patients who have a large excess of skin and fat hanging down over the pubic area. In this procedure only the surplus skin and are removed. The scar is long and transverse extending from one side of the apron to the other.
Modifications to the abdominoplasty skin excision are made when the patient has particular problems associated with scars from previous operations.
An alternative procedure which should always be considered instead of many of the above is liposuction on its own. This reduces fat and causes just a little retraction of the skin.
Who is a candidate?
Anyone who has abdominal skin and fat may be a candidate. With women the problem is usually caused by pregnancy, but is greatly aggravated by weight loss. The muscles of the abdominal wall may be weakened by pregnancy and actually pulled apart in the middle (divarification of recti). Men are similarly affected by weight loss. Stretch marks (striae) are simply the scars which are left after extreme stretching of the skin. They are usually most apparent on the lower part of the abdominal wall. There is no specific treatment for these stretch marks, but many of them are excised in an abdominal reduction and those that are left are tightened making them look less obvious.
Patients that are unable to tighten the abdominal wall skin with exercise or wish to achieve a smoother flatter abdomen will also benefit.
What are the consequences?
The patient is left with noticeable scars. The main scar runs transversely across the lower part of the abdomen (see illustrations above) and in a standard abdominal reduction there will be a scar around the umbilicus. Other or different scars may be left where the patient has particular individual problems. Some patients make better scars than others and in any case all scars are red initially. It is essential that the patient understands where these scars will be and should discuss them with the surgeon. Although we try to hide them beneath underwear and swimwear, fashions can change making previously covered scars visible.
There is numbness in the lower part of the abdominal wall after surgery. This is usually temporary but could be permanent. Swelling above the scar is usually present due to a collection of tissue fluid which normally drains to the groin. This swelling or oedema settles within a few months.
What are the limitations?
The skin is usually tightened downwards and this does not tighten the waist. If this is desired then one can consider removing skin vertically, but one should bear in mind that vertical scars of the abdomen are less good. The tissue of the abdominal wall is generally fatter than the groin and if liposuction is not carried out a fatty bulge may remain above the scar.
The beneficial effects of the operation will last well. However, the effects will be maintained better if the patient keeps exercising the muscles and the weight steady. A further pregnancy will of course stretch the skin again, although probably not to the same degree.
What are the risks?
The standard abdominoplasty is a large procedure requiring two to four days of hospitalisation. Drains are removed when they stop draining blood and serum a few days after the procedure. This fluid can reaccumulate after the drains are removed requiring drainage or aspiration.
Healing can be slow particularly in the tighter central part of the wound and sometimes dressings are needed for a few weeks. This is more common in patients who are overweight and who smoke. This tends to leave more obvious scars which are tethered - these can be revised.
Secondary procedures are sometimes carried out to tidy up the results and will involve scar revision and limited liposuction. Displacement of the umbilicus to one side has been over-publicised and is rare. Deep vein thrombosis and pulmonary embolus are rare complications of any operation, including this one.
What would you need to do before the operation?
If you are overweight you would be well advised to diet as best results are obtained in people who are the correct weight for their height. If you are taking the contraceptive pill you should stop doing so for six weeks before surgery and use an alternative method in order to reduce the risk of thrombosis. If you smoke there is a greater risk of chest infection and in particular healing of the abdominal wound is less good.
What you should expect at the time of the operation
You will need to be in hospital for one to three days. When you wake up for your operation it is likely that you will be having a transfusion of salt solution. This is quite normal and is to provide you with fluid you need whilst you are not drinking. You are likely to have drainage tubes coming out of each side of the lower abdomen which are there to drain any collection of blood or serum. You can expect some moderately severe pain for which you will be given painkilling tablets or injections. You will be asked to keep your knees and hips bent to take the strain off your stitches.
Recuperation
Overactivity in the early days reduces healing and increases fluid accumulation. Light activities are comfortable in 10 to 20 days. Sports will not be possible for about 6 weeks particularly when the muscles have been strengthened with sutures. A corset is usually helpful to reduce the swelling and improve comfort in the first month.
Content used with permission from the British Association of Aesthetic Plastic Surgeons website: Tummy Tuck (Abdominoplasty). Copyright for this leaflet is with the BAAPS.
Disclaimer
This leaflet is designed to supply useful information but is not to be regarded as advice specific to any particular case. It does not replace the need for a thorough consultation and all prospective patients should seek the advice of a suitably qualified medical practitioner. The BAAPS accepts no liability for any decision taken by the reader in respect of the treatment they decide to undertake.
Patient picks for Other surgery and procedures

Surgery and procedures
Weight loss surgery
Weight loss surgery can work well to help some people to lose weight. However, it may not be suitable or the right decision for everyone. It is not something to be undertaken without very careful consideration. You need to be fully prepared for weight loss surgery and you need to be highly motivated. When considering surgery you must have a full understanding of what it involves, including the risks and benefits. You should also be aware that you need to make long-term changes to your lifestyle and eating habits after your surgery. If you have surgery abroad or in the private sector in the UK then you should budget for two years specialist follow-up in the private sector.
by Dr Toni Hazell, MRCGP

Surgery and procedures
Arthroscopy and arthroscopic surgery
Arthroscopy is a surgical procedure which uses a thin telescope with a light source (an arthroscope) to look inside joints. As well as being able to look inside, the surgeon can use an arthroscope to perform keyhole surgery. Arthroscopy is most often used to investigate or treat knee problems. Arthroscopy can also be used for other joints, including the shoulder, hip, elbow, wrist and ankle joints, and even for hand or foot problems. Note: the information below is a general guide only. The arrangements, and the way tests are performed, may vary between different hospitals. Always follow the instructions given by your doctor or local hospital.
by Dr Rachel Hudson, MRCGP
Frequently asked questions
What is an apronectomy, and how is it different from other abdominoplasty procedures?
An apronectomy is a specific type of abdominoplasty designed for patients with a significant excess of skin and fat that hangs down over the pubic area, often referred to as an 'apron.' Unlike some other procedures, it solely focuses on removing this surplus skin and fat, leaving a long, transverse scar from one side of the apron to the other. It doesn't involve repositioning the navel or extensive muscle tightening in the same way a standard abdominoplasty might.
Can abdominoplasty completely remove all my stretch marks?
Abdominoplasty primarily focuses on removing excess skin and fat. While many stretch marks, particularly those on the lower part of the abdominal wall, may be excised along with the skin, some might remain. The remaining stretch marks will be tightened due to the skin reduction, which can make them appear less obvious, but there is no specific treatment for stretch marks themselves.
Will an abdominoplasty help me achieve a tighter waist?
Generally, an abdominoplasty primarily tightens the skin downwards on the abdomen, which typically does not tighten the waist. If tightening the waist is a specific goal, alternative approaches might need to be considered, such as removing skin vertically. However, it's important to note that vertical abdominal scars tend to be less aesthetically pleasing than horizontal ones.
How long will I experience numbness after the surgery?
Numbness in the lower part of the abdominal wall is common after abdominoplasty. This condition is usually temporary, meaning it should resolve over time. However, in some cases, the numbness could become permanent.
What can I do to ensure the best long-term results from my abdominoplasty?
To best maintain the beneficial effects of an abdominoplasty, it is important to continue exercising your abdominal muscles and keep your weight stable. While the procedure's effects are generally lasting, significant weight fluctuations or further pregnancies can stretch the skin again, though likely not to the same extent as before.
What is the typical hospital stay for a standard abdominoplasty?
A standard abdominoplasty is considered a major surgical procedure. Patients can expect to be hospitalised for two to four days following the operation.
Further reading and references
- Calle EE, Rodriguez C, Walker-Thurmond K, et al; Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003 Apr 24;348(17):1625-38.
- Flegal KM, Kit BK, Orpana H, et al; Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013 Jan 2;309(1):71-82. doi: 10.1001/jama.2012.113905.
- Obesity in the UK: A psychological perspective; British Psychological Society, 2011
- Childhood overweight and obesity; World Health Organization
- Oude Luttikhuis H, Baur L, Jansen H, et al; Interventions for treating obesity in children. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001872. doi: 10.1002/14651858.CD001872.pub2.
- MEND; (Mind, Exercise, Nutrition ... Do it!)
- Position statement: Childhood obesity; Royal College of Paediatrics and Child Health, 2012
- Hsia DS, Fallon SC, Brandt ML; Adolescent bariatric surgery. Arch Pediatr Adolesc Med. 2012 Aug;166(8):757-66. doi: 10.1001/archpediatrics.2012.1011.
- Sjostrom L; Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013 Mar;273(3):219-34. doi: 10.1111/joim.12012. Epub 2013 Feb 8.
- Healthy lives, healthy people. A call to action on obesity in England; Dept of Health, 13 October 2011
- Reducing obesity and improving diet: Policy; Dept of Health, March 2013
- Body Mass Index (BMI) charts for girls and boys age 2-18; Royal College of Paediatrics and Child Health and Dept of Health
- Colquitt JL, Pickett K, Loveman E, et al; Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014 Aug 8;8:CD003641. doi: 10.1002/14651858.CD003641.pub4.
- Arterburn DE, Courcoulas AP; Bariatric surgery for obesity and metabolic conditions in adults. BMJ. 2014 Aug 27;349:g3961. doi: 10.1136/bmj.g3961.
- Obese, overweight with risk factors: liraglutide (Saxenda); NICE Evidence Summary, June 2017
- Hafekost K, Lawrence D, Mitrou F, et al; Tackling overweight and obesity: does the public health message match the science? BMC Med. 2013 Feb 18;11:41. doi: 10.1186/1741-7015-11-41.
- About Obesity: Body Mass Index; MEND - Mytime Active
- Yeh JS, Kushner RF, Schiff GD; Obesity and Management of Weight Loss. N Engl J Med. 2016 Sep 22;375(12):1187-9. doi: 10.1056/NEJMclde1515935.
About the authorView full bio

Dr Jacqueline Payne, FRCGP
General Practitioner, Medical Author
MB, BS, DFFP, DRCOG, FRCGP
Jacqueline was a GP in Kendal, Cumbria for 25 years, where she trained young GPs for the RCGP and was an Instructing Doctor for the FSRH.
About the reviewerView full bio

Dr Helen Huins, MRCGP
General Practitioner, Medical Author
MB, BS, Lond, DCH, DRCOG, MRCGP, JCPTGP, DFFP
Helen qualified at Guy’s Hospital in 1989 and left London in 1990 to settle in the countryside.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
24 Mar 2016 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in surgery and procedures
- Anaesthesia
- Anaesthetic for hip or knee replacement
- Arthroscopy and arthroscopic surgery
- Bone marrow biopsy and aspiration
- Breast augmentation
- Breast reduction
- Coronary angioplasty
- Cystoscopy
- Death or brain damage from anaesthesia
- Endometrial biopsy
- ERCP
- Facelifts
- Female sterilisation
- Gastroscopy
- Hip replacement
- Kidney biopsy
- Knee replacement
- Post-dural puncture headache
- Preventing infection after splenectomy
- Weight loss surgery