Spondylolisthesis and spondylolysis
Revisado por pares por Dr Hayley Willacy, FRCGP Última actualización por Dr Philippa Vincent, MRCGPLast updated 20 Nov 2021
Cumple con las directrices editoriales
- DescargarDescargar
- Compartir
- Language
- Discusión
- Versión en audio
- Add to preferred sources on Google
Profesionales Médicos
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Cervical spondylosis article more useful, or one of our other artículos de salud.
En este artículo:
Continúa leyendo abajo
What is spondylolisthesis?
La espondilolistesis es el desplazamiento de una vértebra en relación con las demás en dirección anterior o posterior. Es más común en L5-S1.
Anatomy of the vertebrae
The vertebrae can be divided into three portions:
Centrum - the body of the vertebra, which is involved in weight-bearing, and is formed of cancellous bone.
Dorsal arch - surrounds and protects the spinal cord. It carries the upper and lower facet joints of each vertebra which articulate with the facet joints of the vertebra above and below, respectively. The part of the vertebral arch between them is the thinnest part and is called the pars interarticularis, or the isthmus.
Posterior aspect - protrudes and can be palpated on the lower back.
Lumbar vertebra 1 inferior surface
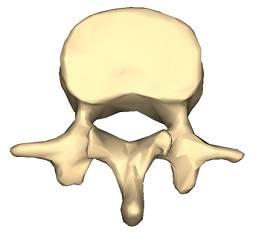
© Anatomography, via Wikimedia Commons
Lumbar vertebra 1 anterior surface
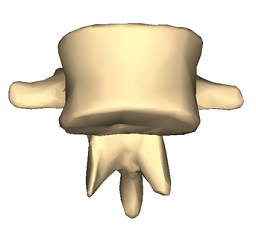
© Anatomography, via Wikimedia Commons
Click here to see a lumbar vertebra 1 close-up superior surface animation.
Types of spondylolisthesis1
Volver al contenidoStable or unstable.
Asymptomatic or symptomatic.
Graded according to degree of slippage; the Meyerding classification is based on the ratio of the overhanging part of the superior vertical body to the anterio-posterior length of the inferior vertebral body:
Grade I: 0-25%.
Grade II: 26-50%.
Grade III: 51-75%.
Grade IV: 76-100%.
Grade V (spondyloptosis): >100%.
Graded according to type; the Wiltse classification (1976):
Type I: dysplastic (congenital).
Type II: isthmic: secondary to a lesion involving the pars interarticularis:
Subtype A: secondary to stress fracture.
Subtype B: result of multiple healed stress fractures resulting in an elongated pars.
Subtype C: acute pars fracture (rare).
Type III: degenerative.
Type IV: post-traumatic: fracture in a region other than the pars.
Type V: pathological: diffuse or local disease.
Type VI: iatrogenic.
Continúa leyendo abajo
Spondylolisthesis vs spondylolysis
Volver al contenidoSpondylolysis and spondylolisthesis are separate conditions, although spondylolysis often precedes spondylolisthesis.
Spondylolysis is a bony defect (commonly due to a stress fracture but it may be a congenital defect) in the pars interarticularis of the vertebral arch, separating the dorsum of the vertebra from the centrum. It may occur unilaterally or bilaterally. It most commonly affects the fifth lumbar vertebra and may cause back pain.
Spondylolisthesis refers to the anterior slippage of one vertebra over another (or the fifth vertebra over the sacrum).
Spondylosis is a general term for degenerative osteoarthritic changes in the spine. There may be changes in the facet joints with osteophyte formation and this may put pressure on the nerve roots, causing motor and sensory disturbance. Spondylosis is seen in around 80% of asymptomatic patients over 50; x-ray findings may not always be the cause of symptoms.2
How common is spondylolisthesis and spondylolysis? (Epidemiology)
Volver al contenidoSpondylolysis is a common diagnosis with a high prevalence in children and adolescents complaining of low back pain.
There is an increased risk of spondylolysis in young athletes like gymnasts, presumably due to impact-related fracturas por estrés. However most cases are low-grade. At-risk activities include gymnastics, diving, tennis, cricket, weightlifting, football and rugby.
La espondilolistesis ístmica afecta aproximadamente al 3-7% de la población, pero es más común en los atletas jóvenes. El 60-80% de las personas con espondilólisis tienen espondilolistesis asociada.3
La mayoría de los casos de espondilólisis y espondilolistesis afectan a L5-S1 y la mayoría del resto afectan a L4-L5.
Degenerative spondylolisthesis is more common in older people, particularly women.
La mayoría de los casos de espondilolistesis son asintomáticos.
Continúa leyendo abajo
Spondylolisthesis causes (aetiology)
Volver al contenidoSpondylolisthesis commonly occurs due to a fracture or defect in the pars interarticularis, the narrowest part of the posterior vertebral arch between the upper and lower facet joints. When this is breached, the upper facet joint may no longer be able to hold the vertebra in place against the downward force of body weight and forward/downward slippage occurs.
Risk factors for spondylolisthesis
Los factores de riesgo que aumentan la probabilidad de que la espondilólisis se desarrolle en espondilolistesis incluyen:
Género femenino.
Edad joven.
Presence of spina bifida or spina bifida occulta.
Vertebral wedging.
Hyperlordosis.4
Positive family history.
Certain high-impact sports, as evidenced by increased rates in athletes and gymnasts.3
Symptoms of spondylolisthesis (presentation)
Volver al contenidoSpondylolisthesis symptoms
Presentation varies slightly by type although common spondylolisthesis symptoms include exercise-related back pain, radiating to the lower thighs, which tends to be eased by rest, particularly in positions of spinal flexion.
Isthmic spondylolisthesis
Most patients are asymptomatic, even with progressing slippage.
Symptoms often begin around the adolescent growth spurt.
Back pain - worse with activity (particularly back extension) - this may come on acutely or insidiously.
Pain may flare with sudden or trivial activities and is relieved by resting.
Pain is worse with higher grades of disease.
Pain may radiate to buttocks or thighs
There are usually no neurological features with lower grades of slippage but radicular pain becomes common with larger slips. Pain below the knee due to nerve root compression or disc herniation would suggest more severe slippage. High degrees of spondylolisthesis may present with neurogenic claudication or even cauda equina impingement.
Tightened hamstrings are very common
There may be enhanced lordosis and a waddling gait with shortened step length.
There may be gluteal muscular wasting.
Degenerative spondylolisthesis
Pain is aching in nature and insidious in onset.
Pain is in the low back and posterior thighs.
Neurogenic claudication may be present with lower-extremity symptoms worsening with exercise.
Symptoms are often chronic and progressive, sometimes with periods of remission.
If lumbar stenosis is also present, reflexes may be diminished.
Dysplastic spondylolisthesis
Presentation and physical findings are similar to isthmic spondylolisthesis but with a greater likelihood of neurological compromise.
Traumatic spondylolisthesis
Patients will have experienced acute trauma and are likely to have significant pain.
Severe slips may cause cauda equina compression with bladder and bowel dysfunction, radicular symptoms or neurogenic claudication.
Physical findings are as for the other types.
Pathological spondylolisthesis
Symptoms may be insidious in onset and associated with radicular pain.
Physical findings are as for the other types.
Spondylolysis symptoms
Most cases of spondylolysis are asymptomatic and identified incidentally.
It may present with low back pain provoked by lumbar extension, paraspinal spasm and tight hamstrings.
It frequently does not show on X-ray. It is important to consider it in the differential diagnosis of back pain, as its identification can prevent progression and avoid the potential need for aggressive intervention.
Diagnóstico diferencial
Volver al contenidoOther causes of back pain need to be ruled out such as:
Spinal cord lesion.
Diagnosing spondylolisthesis (investigations)
Volver al contenidoBlood tests - looking for infection, myeloma, hypercalcaemia/hypocalcaemia.
Lateral spinal X-rays - will show spondylolisthesis. These are best performed in the position of maximal pain.
Oblique spinal X-rays - may (but will often not) detect spondylolysis.
Radionuclide scintigraphy and CT may help in cases of spondylolysis in distinguishing progressing lesions of the pars from stable lesions.
MRI is often performed perioperatively to look at relationships between the bony and neurological structures in the compromised area.
Spondylolisthesis treatment and management
Volver al contenidoEl objetivo del tratamiento es aliviar el dolor, estabilizar el segmento espinal y detener o revertir el deslizamiento. Es importante reconocer que muchas de estas opciones de tratamiento, incluyendo el uso de corsés, fisioterapia temprana e inyecciones de esteroides o bloqueos nerviosos, pueden no estar disponibles en el NHS.
Conservative treatment
El tratamiento conservador generalmente se utilizará primero y hasta el 90% de los atletas con espondilolistesis regresaron a sus actividades dentro de los 6 meses de manejo conservador.5
El tratamiento conservador incluye restringir la actividad, el uso de férulas y el control del dolor mediante medicamentos. Si esto no ha sido exitoso dentro de 2 semanas, normalmente se aconseja la fisioterapia y se recomienda el ejercicio como el ciclismo o la natación para mantener los niveles de condición física sin causar más daño. Se ha demostrado que tratamientos como el uso de férulas y la disminución de la actividad son más efectivos en pacientes con diagnóstico y tratamiento temprano. Si esto no tiene éxito dentro de 6 semanas, se pueden considerar inyecciones epidurales de esteroides o bloqueos nerviosos selectivos.5
Tratamiento quirúrgico
If there is evidence of progression or if conservative measures are ineffective then surgical therapy may be offered. This depends also on degree and aetiology.
Surgical intervention involves a prolonged rehabilitation period so it is generally not considered until conservative treatments have failed. An exception would be in the case of significant instability or neurological compromise and in high-grade slips.
Surgical therapy involves fusing the affected vertebra with a neighbouring normally aligned vertebra (both anteriorly and posteriorly). The intervertebral disc is usually also removed, as it is inevitably damaged. The slipped vertebra may be realigned.
Existen relativamente pocos estudios que analicen los beneficios del manejo quirúrgico, aunque los que existen tienden a mostrar que los pacientes reportan beneficios de la cirugía.5
Complications of surgical repair
Volver al contenidoImplant failure.
Pseudoarthrosis (failure of bone healing leading to a 'false joint').
Poor alignment of the fusion.
Neurological damage: foot drop, compresión de la médula espinal. Chronic nerve injury/inflammation: neuropathic pain can persist in the face of apparent surgical success, possibly due to permanent changes in the nerves or a deregulation of pain control mechanisms.
Pronóstico1
Volver al contenidoEl pronóstico para la espondilolistesis de bajo grado es excelente, con la mayoría de los pacientes permaneciendo asintomáticos o mostrando muy poca progresión con el tiempo. Los niños con espondilosis y espondilolistesis de bajo grado generalmente permanecen estables y los hallazgos en las radiografías pueden volver a la normalidad sin intervención. Los adultos usualmente tienen poca progresión, aunque esto puede ocurrir con cambios degenerativos relacionados con la edad.
La espondilolistesis de alto grado es más difícil de predecir. La progresión es más probable y los adultos a menudo presentan inestabilidad mecánica significativa, desalineación sagital y síntomas neurológicos. Es más probable que necesiten intervención quirúrgica, aunque el riesgo de complicaciones significa que esto requiere una planificación cuidadosa.
La Dra. Mary Lowth es una autora o la autora original de este folleto.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Política de Privacidad. Puedes darte de baja en cualquier momento. Nunca vendemos tus datos.
Lecturas adicionales y referencias
- Margetis K, Gillis CC; Spondylolisthesis.
- R Prasath et al.; Espondilosis Lumbar: Presentación Clínica y Enfoques de Tratamiento – Una Revisión Sistemática. Journal of Pharmaceutical Negative Results, Volumen 13, Edición Especial 9, 2022
- Espondilólisis: Una Revisión Narrativa de Etiología, Diagnóstico y Manejo; V Madden et al; Revista Internacional de Investigación Ambiental y Salud Pública
- Hyperlordosis.
- Li N, Scofield J, Mangham P, et al; Espondilolistesis. Rev Ortop (Pavia). 27 de julio de 2022;14(3):36917. doi: 10.52965/001c.36917. eCollection 2022.
Continúa leyendo abajo
About the authorView full bio

Dra. Philippa Vincent, MRCGP
Médico General, Autor Médico
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dra Philippa Vincent is an NHS GP working in North London.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
Médico General, Autor Médico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Historial del artículo
La información en esta página está escrita y revisada por pares por clínicos calificados.
Próxima revisión: 19 Nov 2026
20 Nov 2021 | Última versión

Pregunta, comparte, conecta.
Navega por discusiones, haz preguntas y comparte experiencias en cientos de temas de salud.

¿Te sientes mal?
Evalúa tus síntomas en línea de forma gratuita