Oclusiones de la vena retiniana
Revisado por pares por Dr Doug McKechnie, MRCGPÚltima actualización por Dr Philippa Vincent, MRCGPÚltima actualización 22 Dic 2024
Cumple con las directrices editoriales
- DescargarDescargar
- Compartir
- Language
- Discusión
- Versión en audio
- Agregar a fuentes preferidas en Google
Profesionales Médicos
Los artículos de Referencia Profesional están diseñados para ser utilizados por profesionales de la salud. Están escritos por médicos del Reino Unido y se basan en evidencia de investigación, así como en guías del Reino Unido y Europa. Puede encontrar el Oclusión de la vena retiniana artículo más útil, o uno de nuestros otros artículos de salud.
¿Qué son las oclusiones de las venas retinianas?
Retinal vein occlusions (RVOs) are the second most common type of retinal vascular disorder after diabetic retinal disease.1 Pueden ocurrir a casi cualquier edad (aunque típicamente ocurren en la mediana edad o en años posteriores - la mayoría en personas mayores de 65 años) y su gravedad varía desde asintomáticos hasta un ojo doloroso con deterioro visual severo.
Retinal vein occlusion is one of the most common causes of sudden painless unilateral loss of vision. Loss of vision is usually secondary to macular oedema. Occlusion may occur in the central retinal vein or branch retinal vein.2
Fisiopatología
Central retinal vein occlusion (CRVO) can be divided into ischaemic CRVO and non-ischaemic CRVO. Non-ischaemic CRVO is more common, accounting for 75% of cases.34
Occlusion of the retinal venous system by thrombus formation is the most common cause but other causes include disease of the vein wall and external compression of the vein. Retinal arteries and arterioles and their corresponding veins share a common adventitial sheath. It is thought that the thickening of the arteriole compresses the vein, eventually causing occlusion.
A backlog of stagnated blood combined with associated hypoxia results in extravasation of blood constituents, causing further stagnation and so on, resulting in the creation of a vicious circle of events. Ischaemic damage to the retina stimulates increased production of vascular endothelial growth factor (VEGF) which, in turn, may lead to neovascularisation - a process that can result in haemorrhage (as the new vessels are of poor quality) or neovascular glaucoma (the new vessels grow into the aqueous drainage system, so clogging it up). Factors contributing to this pathophysiology include:
Advancing age.
Systemic conditions such as hypertension (found in 64% of patients with RVO), hyperlipidaemia, diabetes, smoking and obesity.
Raised intraocular pressure.
Inflammatory diseases such as sarcoidosis, Behçet's syndrome.
Hyperviscosity states such as myeloma.
There are more unusual associations, including chronic kidney disease, other secondary causes of hypertension and diabetes (eg, Cushing's syndrome), secondary causes of hyperlipidaemia (eg, hypothyroidism), polyarteritis nodosa, granulomatosis with polyangiitis, Goodpasture's syndrome.
Branch retinal vein occlusion
Branch retinal vein occlusions (BRVOs) are three times more common than central retinal vein occlusions (CRVOs). There are various subclassifications of this depending on whether a major branch, a minor macular branch or a peripheral branch is affected. Each carries its own prognosis. A hemiretinal vein occlusion refers to an occlusion that is proximal enough to affect half of the retinal drainage (ie the superior or inferior portion) as opposed to the smaller portion affected by a BRVO.
Presentación
This largely depends on the amount of compromise to macular drainage. The most common presentation is of unilateral, painless blurred vision, metamorphopsia (image distortion) ± a field defect (usually altitudinal). Peripheral occlusions may be asymptomatic. Visual acuity depends on the degree of macular involvement. Fundoscopy will reveal vascular dilatation and tortuosity of the affected vessels, with associated haemorrhages in that area only (look for an arc of haemorrhages, like a trail left behind a cartoon image of a shooting star).
Manejo
Urgent referral to an on-call ophthalmologist.
Management depends on the area and degree of occlusion.
Some patients benefit from panretinal photocoagulation (PRP) laser treatment if they develop macular oedema (where visual acuity is ≤6/12 and there is no spontaneous improvement by 3-6 months) or neovascularisation.
Triamcinolone is no longer recommended for the treatment of macular oedema in BRVO.
Dexamethasone biodegradable implants are licensed for treatment of macular oedema secondary to BRVO.
Use of the anti-vascular endothelial growth factor (anti-VEGF) ranibizumab has been shown to have sustained benefit for macular oedema resulting from BRVO. The National Institute for Health and Care Excellence (NICE) recommends that it should be used only if treatment with laser photocoagulation has not been beneficial, or when laser photocoagulation is not suitable because of the extent of macular haemorrhage.5
Complicaciones
These are similar to those of CRVO. New vessels tend to occur only when at least one quadrant of the retina is affected, and appear about six months after the original occlusion. The rate of complication for hemiretinal vein occlusions is greater than that of BRVO but less than that of CRVO.
Resultado
The outcome is reasonably good depending on the number of collateral veins that develop. 50% of patients return to a visual acuity of 6/12 or better. Over half will develop macular oedema and about one in five may develop retinal neovascularisation.
Central retinal vein occlusion
CRVO has two broad categories, which may overlap:
La forma más leve de la enfermedad es OVCR no isquémica (accounting for ~75% of CRVOs). This may resolve fully with good visual outcome or progress to the ischaemic type.
La forma grave de la enfermedad es ischaemic CRVO. Patients may be left with neovascular glaucoma and a painful eye with severe visual impairment.
In some cases, the cut-off between the two can be arbitrarily based on angiographic findings but it is a useful predictor of outcome and complication development.
How common is central retinal vein occlusion? (Epidemiology)
This is a common condition. UK figures are not available. The prevalence of central vein retinal occlusion has been reported to be 0.8 per 1000 people in the developed world.3 La incidencia aumenta con la edad. Hay una distribución equitativa entre sexos.
Presentación
The patient (usually aged >50) frequently presents with sudden unilateral painless loss of vision or blurred vision, often starting on waking.2
Non-ischaemic - defecto pupilar aferente leve o ausente. Hay hemorragias puntiformes y en llama generalizadas en todo el fondo de ojo y algo de edema de disco.
Isquémico - deterioro visual severo con un defecto pupilar aferente marcado. El fondo de ojo se parece a la imagen no isquémica, pero el edema del disco es más severo. Hemorragias dispersas por todo el fondo de ojo en un patrón típico de tormenta de sangre con manchas algodonosas (hemorragias dispersas escasas con un bloqueo menos completo). Ocasionalmente puede haber un desprendimiento de retina asociado.4
Branch retinal vein occlusion
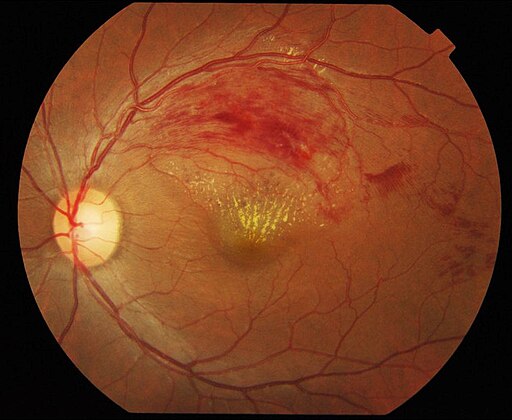
© Ku C Yong, Tan A Kah, Yeap T Ghee, Lim C Siang and Mae-Lynn C Bastion, Department of Ophthalmology, Universiti Kebangsaan Malaysia Medical Centre (UKMMC) and Universiti Malaysia Sarawak (UNIMAS), Kuala Lumpur, Malaysia., CC BY 2.0, via Wikimedia Commons
Diagnóstico diferencial
Diabetic retinopathy.
Otras causas de pérdida súbita de visión unilateral - por ejemplo, desprendimiento de retina, oclusión de la arteria retiniana.
Otras causas de edema macular.
Manejo
Currently, there are no proven treatment options available so management has the twofold aim of identifying/managing modifiable risk factors and recognising/treating complications. Where there is development of severe visual impairment due to a secondary complication (eg, neovascular glaucoma), the management aim is to keep the eye pain-free.
Urgent referral to the on-call ophthalmologist.
Investigations will include:3
Blood pressure.
Blood tests including ESR, FBC, lipid profile, blood glucose, renal function and thyroid function.
ECG (looking for LVH).
Patients under the age of 50 or with bilateral RVO or a family history should also be offered:3
Chest x-ray (looking for sarcoidosis or tuberculosis).
CRP, auto-antibodies, serum ACE levels, syphilis screen, serum homocysteine levels.
Thrombophilia screen.
Carotid duplex imaging.
The ophthalmologist will seek certain features that distinguish ischaemic from non-ischaemic CRVO. The former will be observed every 2 to 3 months ± treated with laser (panretinal photocoagulation) should any neovascularisation - particularly around the iris - occur.
Reduction of intraocular pressure is needed if this is elevated.
Intravitreal anti-VEGF agents:
In combination with use of laser panretinal photocoagulation (PRP), should be used when iris new vessels or angle new vessels are visible.
PRP results in dramatic regression of the new vessels. The effect is short-lived and new vessels recur commonly, so repeated treatment (typically every six weeks) with these agents (and PRP) may be required.
Intravitreal aflibercept injection is recommended as an option for treating visual impairment caused by macular oedema secondary to CRVO.6
Intravitreal triamcinolone has been evaluated but its beneficial effects in CRVO are short-lived and it is rarely offered as a treatment currently.
Intravitreal steroids have also been studied with regard to treating post-CRVO macular oedema. Currently, the response has been found to be positive but limited temporally and there are a number of complicating side-effects.7
Laser-induced chorioretinal venous anastomosis (L-CRA) has been used as a treatment for non-ischaemic CRVO. Improvements in laser technology have led to higher success rates in L-CRA creation and a reduction in complications.8
Any underlying modifiable risk factors will need to be identified and addressed.
Complicaciones
Retinal neovascularisation (and secondary glaucoma or vitreous haemorrhage - the '90-day glaucoma').
Edema macular ± agujero macular lamelar o de espesor completo.
Permanent macular degeneration or 'cellophane maculopathy'.
Resultado
The prognosis in central retinal vein occlusion is best in patients under the age of 50. In patients over 50, one third improve, one third stay the same and one third deteriorate.3
In non-ischaemic retinal vein occlusion, about 50% return to baseline or near-baseline visual acuity. Chronic macular oedema is the main cause of ongoing visual loss. The prognosis is usually linked to the initial visual acuity on diagnosis. Patients with initial visual acuity of 20:60 or better, normally stay the same. Patients with an initial visual acuity of 20:200 or worse, also usually stay the same and rarely improve, Patients with an initial visual acuity between these have a more variable clinical course with some improving, some worsening and some staying the same.3
In ischaemic retinal vein occlusion, the prognosis is more variable. 50% will develop glaucoma in the first 2-4 months. Less than 5% will re-vascularise.3
There is no risk of increased long-term mortality (in contrast to retinal artery occlusion). However, there is a risk of developing CRVO in the fellow eye.
Investigaciones
In the eye clinic, further evaluation includes:
Measurement of intraocular pressure.
Fluorescein angiography is the investigation of choice in CRVO. It evaluates retinal capillary non-perfusion, neovascularisation and macular oedema. It is not often necessary in BRVO.
Optical coherence tomography angiograph (OCTA). This is non-invasive, transpupillary imaging. It measures the retina and can detect macular oedema that fluorescein angiography has missed because of blockage from haemorrhage.9
Non-ophthalmological management of retinal vein occlusions
El equipo de oftalmología se ocupa principalmente del diagnóstico de RVO y del manejo de las complicaciones oculares. Las investigaciones iniciales deben ser realizadas por el equipo de oftalmología en el momento del diagnóstico.
It is also their responsibility to impart this information effectively to the patient's GP, as underlying risk factors need to be assessed and addressed urgently. Rarer causes (such as those encountered in younger patients) need managing by relevant specialists. Initiation of medical management should occur within two months of diagnosis.
Los factores de riesgo han sido identificados en 'Fisiopatología', arriba. El área principal de investigación y manejo serán los factores de riesgo cardiovascular. Ver el apartado separado Prevención de enfermedades cardiovasculares artículo.
Issues which may arise in the context of general practice
Terapia de reemplazo hormonal (TRH) - históricamente, la THS estaba contraindicada y se suspendía en mujeres que experimentaban un RVO. Sin embargo, estudios más recientes han demostrado que el uso continuado no parece estar asociado con una mayor tasa de recurrencia. Además, se cree que el estrógeno transdérmico no aumenta el riesgo de eventos trombóticos. Anteriormente, se aconsejaba reiniciar la THS caso por caso, pero no se recomendaba comenzar la THS de novo. Con el uso creciente de estrógeno TD, esto puede estar cambiando y se debe buscar asesoramiento caso por caso.
The management of younger patients - aunque el resultado visual en este grupo de pacientes parece ser mejor, los RVO están asociados con condiciones sistémicas subyacentes que deben ser manejadas adecuadamente. En mujeres, la asociación más común es con la píldora anticonceptiva oral. Por lo tanto, un RVO es una contraindicación para esto. A veces, no se puede encontrar una causa subyacente a pesar de investigaciones extensas - este grupo presenta un problema de manejo y es probable que esté bajo observación oftalmológica por un período de tiempo mucho más largo.
Actualizaciones exclusivas para profesionales de la salud
Mantente informado con las últimas actualizaciones clínicas, perspectivas profesionales y orientación basada en evidencia. El boletín de Patient Pro selecciona contenido esencial para profesionales de la salud, entregado directamente en tu bandeja de entrada.
Al suscribirte aceptas nuestros Política de Privacidad. Puedes darte de baja en cualquier momento. Nunca vendemos tus datos.
Lecturas adicionales y referencias
- Aflibercept for treating visual impairment caused by macular oedema after branch retinal vein occlusion; NICE Technology appraisal guidance, September 2016
- Blair K, Czyz CN; Oclusión de la Vena Central de la Retina.
- Central Retinal Vein Occlusion; Columbia Ophthalmology
- Esmaili DD, Boyer DS; Recent advances in understanding and managing retinal vein occlusions. F1000Res. 2018 Apr 16;7:467. doi: 10.12688/f1000research.12886.1. eCollection 2018.
- Blair K, Czyz CN; Central Retinal Vein Occlusion. StatPearls 2020.
- Blair K, Czyz CN; Oclusión de la Vena Central de la Retina.
- Central Retinal Vein Occlusion; Columbia Ophthalmology
- Ranibizumab for the treatment of diabetic macular oedema; NICE Technology Appraisal Guidance, February 2013 - last updated October 2023
- Aflibercept for treating visual impairment caused by macular oedema secondary to central retinal vein occlusion, NICE Technology appraisal guidance, February 2014
- Gewaily D, Greenberg PB; Intravitreal steroids versus observation for macular edema secondary to central retinal vein occlusion. Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD007324. DOI: 10.1002/14651858.CD007324.pub2
- McAllister IL; Chorioretinal Anastomosis for Central Retinal Vein Occlusion: A Review of Its Development, Technique, Complications, and Role in Management. Asia Pac J Ophthalmol (Phila). 2020 May-Jun;9(3):239-249. doi: 10.1097/APO.0000000000000286.
- Tsai G, Banaee T, Conti FF, et al; Optical Coherence Tomography Angiography in Eyes with Retinal Vein Occlusion. J Ophthalmic Vis Res. 2018 Jul-Sep;13(3):315-332. doi: 10.4103/jovr.jovr_264_17.
Sobre el autorVer biografía completa

Dra. Philippa Vincent, MRCGP
Médico General, Autor Médico
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dra Philippa Vincent es un médico de cabecera del NHS que trabaja en el norte de Londres.
Acerca del revisorVer biografía completa

Dr Doug McKechnie, MRCGP
Redactor Médico
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
El Dr. Doug McKechnie es un médico de cabecera del NHS que trabaja en Londres. Trabaja a tiempo completo en la práctica clínica y también es el Subdirector del módulo de Práctica Clínica y Profesional en la Escuela de Medicina del University College London.
Historial del artículo
La información en esta página está escrita y revisada por pares por clínicos calificados.
Artículo también disponible en Inglés, Alemán, Español, Francés, Italiano, Portugués, Hindi, Hebreo, Árabe, y Sueco.
Próxima revisión: 21 Dic 2027
22 Dic 2024 | Última versión

Pregunta, comparte, conecta.
Navega por discusiones, haz preguntas y comparte experiencias en cientos de temas de salud.

¿Te sientes mal?
Evalúa tus síntomas en línea de forma gratuita
Más en oftalmología
- Preparaciones oculares antimicrobianas
- Birdshot retinochoroidopathy
- Visión borrosa
- Visión del color y sus trastornos
- Conjuntivitis
- Microquistes corneales
- Problemas corneales - agudos y no agudos
- Epiphora
- Mancha retiniana de Förster-Fuchs
- Síndrome de Foster Kennedy
- Conjuntivitis infecciosa
- Queratoplastia
- Síndrome de Lowe (oculo-cerebro-renal)
- Tumores del nervio óptico y del ojo
- Síndrome de erosión corneal recurrente
- Ojo rojo
- Desprendimiento de retina
- Corrección quirúrgica de errores refractivos
- Verteporfina y otros citotóxicos para el ojo